Episode 28 - Extremity Compartment Syndrome
Learning Objectives
By the end of rounds you should be able to:
1. Describe the pathophysiology of acute extremity compartment syndrome
2. Recognize risk factors and key clinical features of compartment syndrome, namely the 6Ps
3. Understand how to measure and interpret compartment pressures
4. Discuss management considerations and pitfalls re: fasciotomy
Take Home Points
Extremity compartment syndrome is an acute surgical emergency that required a HIGH INDEX OF SUSPICION
Although commonly associated with fractures (especially, tib-fib and distal forearm), up to 1/3 of patients have NO LONG BONE FRACTURE
Pain out of proportion or on passive stretching of a muscle group and paresthesias are the first signs of extremity compartment syndrome
Physical exam, specifically, feeling for the tenseness of a compartment is UNRELIABLE
In the leg, the ANTERIOR and DEEP POSTERIOR compartments are the most frequently missed!
If you suspect it, DO SOMETHING = either a compartment pressure check OR fasciotomy
Time Stamps
00:12 Introduction
02:45 Learning Objectives
03:32 Pathophysiology of Extremity Compartment Syndrome
06:19 Starling’s Hypothesis
09:32 Risk Factors for Extremity Compartment Syndrome both Direct & Indirect
13:41 6Ps (Pain out of proportion and/or with passive motion, Paresthesias, Pallor, Poikilothermia, Paralysis, Pulselessness)
15:46 The Physical Exam for Diagnosing Extremity Compartment Syndrome SUCKS!
17:47 A Prospective Study to Support the Statement Above
19:18 Performing an Intracompartmental Pressure Check
21:42 Use the Differential Pressure NOT Absolute Compartment Pressures
(P diastolic - P compartment < 30mmHG = ABNORMAL)
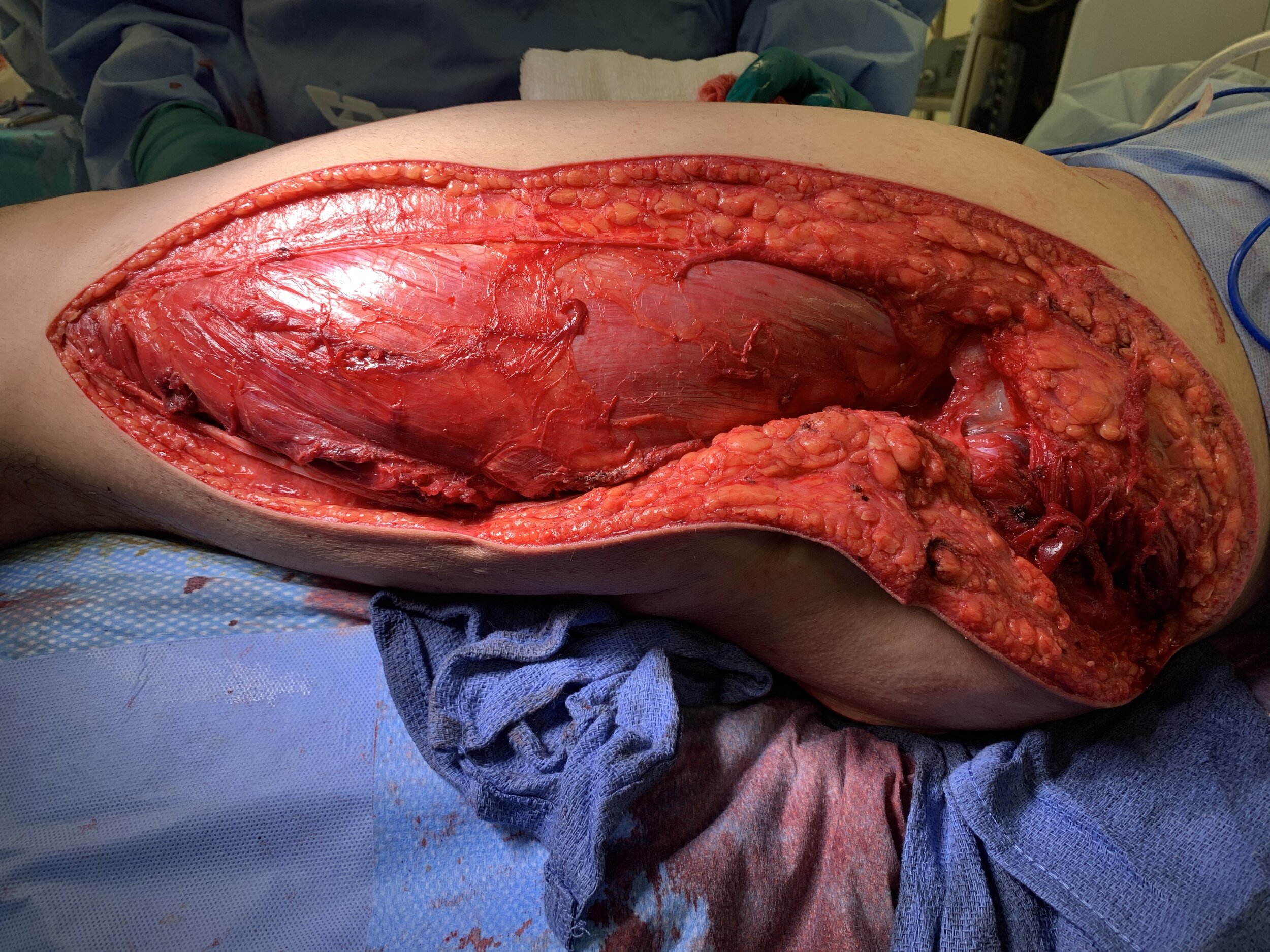
22:46 Performing Fasciotomies (with a focus on the leg)
25:29 Prophylactic versus Therapeutic Fasciotomy: Who, When, Why?
27:53 Wound Care & Postoperative Considerations
28:28 Rhabdomyolysis
29:48 Take Home Points
30:59 Outro & Call to Action
Core Concepts, Equations, and Other Stuff

Recommended Reading
Articles
Brown CV, Rhee P, Chan L, Evans K, Demetriades D, Velmahos GC. Preventing renal failure in patients with rhabdomyolysis: do bicarbonate and mannitol make a difference? J Trauma. 2004 Jun;56(6):1191-6. doi: 10.1097/01.ta.0000130761.78627.10. PMID: 15211124.
Schellenberg M, Chong V, Cone J, Keeley J, Inaba K. Extremity compartment syndrome. Curr Probl Surg. 2018 Jul;55(7):256-273. doi: 10.1067/j.cpsurg.2018.08.002. Epub 2018 Aug 23. PMID: 30470346.
Shuler FD, Dietz MJ. Physicians' ability to manually detect isolated elevations in leg intracompartmental pressure. J Bone Joint Surg Am. 2010 Feb;92(2):361-7. doi: 10.2106/JBJS.I.00411. PMID: 20124063.
von Keudell AG, Weaver MJ, Appleton PT, Bae DS, Dyer GSM, Heng M, Jupiter JB, Vrahas MS. Diagnosis and treatment of acute extremity compartment syndrome. Lancet. 2015 Sep 26;386(10000):1299-1310. doi: 10.1016/S0140-6736(15)00277-9. Erratum in: Lancet. 2015 Nov 7;386(10006):1824. Appelton, Paul T [corrected to Appleton, Paul T]. Erratum in: Lancet. 2015 Nov 7;386(10006):1824. PMID: 26460664.
Websites
Starling’s Hypothesis: https://www.anaesthesiamcq.com/FluidBook/fl4_2.php